
Cross-linking is an innovative treatment of keratoconus and corneal ectasia. With the English term cross linking is the formation of cross-links. The cornea is made up of collagen fibers arranged in an orderly manner: the mechanical strength of the cornea is in relation to the number of fibers and, in particular, to the number of chemical bonds that exist between them (bridge links).

In keratoconus, there is a weakening and an alteration of these bonds where the cornea loses its mechanical strength and tends to progressively deform under the action of intraocular pressure. We currently have two (2) different techniques for cross linking:
- standard corneal cross linking
- transepithelial cross linking
Standard Corneal Cross-Linking
Standard corneal cross linking is a keratoconus therapy that makes the cornea more rigid by stimulating the formation of bonds between collagen fibers, to prevent splintering and subsequent perforation. It is a painless treatment, little invasive, and less than an hour long. It consists of reacting a photosensitive substance, riboflavin or vitamin B2, with ultraviolet light. The patient is instilled at first with an eye drop that tightens the pupil and then applies a second anesthetic eye drop. The epithelial layer that covers the cornea is removed and then the cornea absorbs water with riboflavin, repeating the operation every 3 minutes for about a quarter of an hour. In this way, you are sure that the cornea has absorbed the substance well. Next, the UV radiates the cornea for 30 minutes, continuing to cover it with the riboflavin solution. At the end of the treatment, the cornea is treated with a protective contact lens, leaving it for 3-5 days until complete epithelialization.
Transepithelial Cross Linking

The transepithelial cross linking technique is carried out without the removal of the corneal epithelium, which is the thin layer of cells that covers the cornea. The riboflavin used in this technique contains particular molecules that allow it to penetrate inside the cornea and cross the epithelial layer. This is a non-invasive treatment and very well tolerated by the patient. After the first phase in which the cornea has to absorb the riboflavin repeatedly, a tool is used to keep the eye open (blepharostat). After that, the eye is radiated with low intensity ultraviolet rays (they are not harmful to the eye) for about 30 minutes at 5 minute intervals.
Contraindications To Cross Linking
Among the contraindications to corneal cross linking, we have:
- Corneal thickness that must be at least 400 microns
- Unperforated cornea
- Patient should not have suffered herpetic keratitis in the past,
- Patient should not have any ongoing infections
- Must have no serious eye damage
Other: CCL, C3-R, CCR, KXL, CXL
Transepithelial cross-linking in March 2013 on a patient at the age of 38
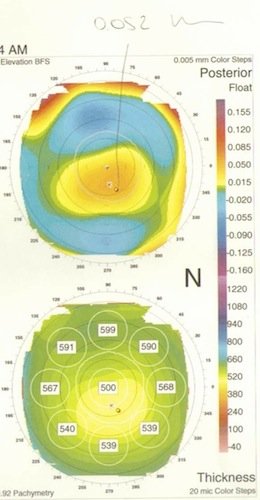

The checkup performed after 6 months highlights a marked improvement in the condition. In particular, the back of the cornea (the one into the inside of the eye) flattened from a 52 micron elevation to 25 (top image). It should be noted that keratoconus begins from the inner area of the cornea. Another improvement noted was the increase in corneal thickness (bottom image)! Pachymetry ranges from 500 to 513 microns. It should also be noted that in keratoconus, the cornea becomes increasingly thin. Cross linking then gives good results and in association with iontophoresis, even better results can be obtained due to the increased absorption of riboflavin by the cornea.